Skin Care & Infant Skin

The combination of experiences with my own children’s skin, and more recently my grandchildren’s skin has inspired this article, and during the research, led me to believe that there is an increasing level of sensitivity in children’s skins in general due to a variety of reasons.
Adult skin differs from infant skin in many ways; however, it is often treated as adult skin because of the belief that a child is simply an adult in miniature. This could not be further than the truth because of the different chemistry and biomechanics of children’s skin.
It is not uncommon to find skin disorders that are characteristic of infancy different in clinical appearance from the adult version of the same problem. With this in mind, it is imperative that a greater understanding of children’s skin and their individual needs for the future is required by both parents and skin care professionals.
Infants and adults contrast greatly from each other in many respects, not because they are an adult reduced in size, but because they are an individual in the initial stages of growing and developing to maturity. The skin of an infant undergoes fundamental changes during the process of growth, this being exemplified by the difference at two stages of development: typically at childhood, the skin appears fresh and soft, while puberty, it is often blemished and oily.
In this article, I will try to describe in simple terms the physiological characteristics of infant skin and its difference from the skin of adults. For the purposes of this discussion, the term “newborn” refers to babies from birth to four weeks, and “infant” refers to children from four weeks to six years old.
Characteristics of infant skin
One of the major differences between infant and adult skin is the composition of the hydrolipic film, which is formed by two groups of lipids and two groups of water.
It is the distinctions in the chemical content between the infant and adult hydrolipic film and the difference in the amount of total skin lipid production at various ages, which dictates the skin care that is required.
Lipid content:
Lipids from the sebaceous glands (sebum) and epidermal lipids found in the bilayers of the stratum corneum (which are formed during the keratinisation process) are included in the formation of this hydrolipic film as are the appcrine and eccrine secretions and the natural moisturising factor (NMF), also part of the bilayers of the stratum corneum.
Lipids secreted from the sebaceous glands (sebum) contain the chemical components triglycerides, free fatty acids, wax esters, sterols and squalene.
Lipids secreted from the epidermis consist of cholesterol, cholesterol esters, phospholipids, triglycerides, sphingolipids, N-Alkanes, squalene and ceramides, all playing an important role in the water retention capabilities of the stratum corneum.
In infants, skin surface lipids consist mainly of the lipids secreted from the sebaceous glands. In general, the total skin lipids of newborns are comparatively close in quantity to those of adults, but they do not contain the same proportion of individual lipids.

Research has shown that total skin lipids decrease during the period from birth to age seven or eight years and after adolescence.
The research revealed a change in chemical components as age increased, typically cholesterol secreted from the epidermis being low in quantity in the newborns, increasing at the ages between four to eight and decreasing thereafter. Conversely, squalene, wax esters and triglycerides secreted by the sebaceous glands are richly present in newborns, tending to decrease during progressing infancy.
The reason for this abundance of sebaceous lipids early in life is that of protection for the body from external stimulus or foreign bodies in foetal life, and after birth reducing as hormonal controls take over. Some reports have shown that boys usually produce more sebum than girls, a theory being the hormones secreted by the newborn causing influence.
As a child moves through infancy, the sebaceous glands under control of hormones secrete less sebum, resulting in drier skin, however during adolescence, when the sex hormones begin activity, sebum secretion capacity increases.
Water content:
We know that the skin has the function of retaining water, and the stratum corneum, the outermost layer of the skin, protects the body from external, physical and chemical influences.
From a skin care point of view, any change in the water content of the stratum corneum is a considered a very important factor.
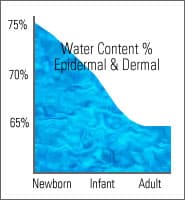
Research has shown the water content of the whole skin (epidermis & dermis combined) reaches 74.5% in newborn babies, 69.4% in infants and 64% in adults.
This research confirms that the water content both in the epidermis and the dermis is much greater in newborns and infants than in adults. Other reports explain that, water content differs between the outer layers and the inner layers within the stratum corneum, and that this difference is important for correct skin care.
Perspiration and infant skin:
The appcrine and eccrine (sweat) glands of the body are completely formed at about the 28th week of embryonic development.
This shows us that the number of sweat glands of newborn babies is identical to that of adults. However, the number of glands per unit area (example: in the thigh) averages 120 per square centimetre in adults and about 500per square centimetre in infants, revealing a greater concentration of sweat glands in infants because of their smaller skin surface.
Sweat glands are present in newborn babies, but their secreting capacity is very low, taking approximately two years to become fully functional.
Sweating is accelerated by exposing the eccrine glands to stimulants such as external temperature, emotionality and taste sensation.
Some newborns demonstrate premature development of sweating, in which they are unable to regulate external conditions, temperature rise or sudamina.

Ph Value: The pH value of a balanced skin is generally between 5.5 and 6.2 and in adults is variable on climatic and ethnic eating habits.
However, the value is close to neutral for the first two weeks after birth, due to the influence of foetal lipids. The pH of placenta is about 7.4. From this, it can be assumed that, in newborns, the skin’s ability to control growth of micro-organisms is not sufficient and, accordingly resistance to infections is low.
Infant skin disorders, potential causes, and remedial measures.
Diaper Dermatitis:
This common problem often manifests itself in one or more of the following; erythema, papules, odema and occasionally erosion. It is generally caused by prolonged contact with the diaper, and in all cases, is accompanied by itching.
Recent research has shown that diaper dermatitis may be attributable to water-soluble substances that are found in faeces. These substances being more irritant than enzymes such as protease or lipase.
The ammonia theory of former times, to the enzymes in the faeces theory of the 90s, give supposition to other causes of dermatitis, and the pros and cons of cloth nappies verses disposables must be considered for many reasons.
While disposable nappies have strong urea absorption power and good air permeability, they should still be changed frequently and baby’s buttocks kept clean by wiping them, or washing them with each change. This is necessary because the fragrance agents so often permeated into the fabric of disposables may be a major aggravating factor on many skins, as are some baby wipes, which are also highly perfumed.
Fragrance in its many forms, is known to be the single causative agent of skin irritation in adult skins, so it stands to reason that a younger, more sensitive skin will be likely to be irritated more readily. A generation ago, it was found that strong detergents found in washing powders would reside in cloth nappies, and insufficient rinsing after washing would result in diaper dermatitis.
With this in mind, I believe that there may be more mechanical causes of dermatitis than we have been previously led to believe.

Miliaria (Prickly heat):
Miliaria is one of the skin disorders characteristic to infants, who because of their undeveloped sweat glands, do not have sufficient temperature control functions in their skin.There are two classifications of miliaria, Miliaria crystallina and Miliaria rubra.
Miliaria crystallina is considered one of the typical disorders of newborns, and is best described as sweat retention in the stratum corneum. It appears as clusters of minute blisters of less than 1mm in diameter, generally on the forehead. In babies, this form often occurs after about one week after birth.
Miliaria rubra, also a disorder of newborns, shows symptoms of a red halo, which is irritated by the constituents of the babies sweat. Common sites are the neck, upper chest, upper limbs, abdomen and inguinal (lower front of abdomen) region. It very often appears around the second week after birth, is very itchy and subsequently susceptible to secondary infection from scratching and irritation.
The most effective measure to relieve these two conditions is the reduction of temperature and humidity of the baby’s room. In the short term however, washing off or absorbing the child’s sweat regularly is also recommended.
Be aware that many modern synthetic fabrics are not always designed for the task of absorption, and often contribute to aggravating prickly heat.
The old fashioned theory of cotton, wool, or silk still stands for baby vests or clothing that has a direct contact with the skin. These fabrics are able to absorb body sweat more readily than many synthetics, hence their continuing popularity with the astute mother.

Talcs and creams although popular through advertising, are not the answer to the problem after the lesions have appeared. Common sense will dictate the best course of action.
With the ever-increasing plethora of inexpensive and imported brands of baby care products on the shelves today, the quality of the ingredients of many must be questioned. If applied to lesions, they may give rise to secondary infection or irritation from the fragrance.
In a worst-case scenario, in addition to irritating and infecting the skin, the product may occlude the skin, reduce its ability to breathe and therefore compound the original condition.
Sebaceous Dermatitis:
This disorder often appears on the head, eyebrow or face where abundant sebaceous secretion is found. It typically occurs after one or two months, or at most within the first four months after birth. The lesions appear to show erythema, are covered by pink oily squama, and have a mild itch.
The causes of sebaceous dermatitis are theorised to include abnormal sebaceous gland function, abnormal vitamin metabolism, and an imbalance between sebaceous excretion and sweating.
It could be easily assumed from a western skin care point of view, that sebaceous dermatitis is due to insufficient washing.
However, it is interesting to note that traditional Japanese procedures for baby care do not include washing of their infant’s with soap.
It is certainly necessary to practice daily bathing procedures with non alkaline soaps or bathing lotions specifically designed for newborn skins, these however are difficult to find and often expensive.
As mentioned previously, less expensive products are often highly perfumed, or if claimed to be fragrance free, have masking agents in them. Baby oils cannot be considered suitable because of the mineral oil content and slight occlusive effect they have on the skin.
Again, this occlusion may have the effect of aggravating the original condition.
Lecithin oil or an oil with a high phospholipid content would be a more suitable choice for softening of the oily squama, and by nature of its composition is more compatible to the skins own lipidic content. Always conclude with a cleanser that has a mild surfactant property to remove the oil.

Actopic Eczema:
Eczema is a dermatitis type tissue reaction involving the epidermis and the upper layers of the dermis. It is caused by external contact with substances to which the skin is allergic, and internal stimulus via allergens in the bloodstream.
Research has shown definite hereditary links and some infants have a cows milk intolerance which appears to be an aggravating factor.
Actopic eczema can affect the skin from birth, the skin inflammation often beginning between 1 to 4 months of age. At this stage of development the disorder is often labelled Infantile Eczema.
This form of dermatosis usually clears by the age of 2 to 3 years, but may re-occur at intervals, later in life. During childhood the dermatosis occurs mostly in the folds of the knees and elbows, or around wrist and ankles. The face and neck usually improve, but the condition may continue behind the ears and around the eyes.
Identifying and avoidance of any potential or known irritant is vital in prevention of actopic eczema. Because of the nature of this condition, and its itchy and weeping effects, it is prone to secondary infection.Keeping the affected areas dry and avoiding scratching or rubbing the affected area is important, however this is difficult to do with newborns or irritable infants.
Again, natural fabrics will help reduce any external rubbing or irritation of the affected areas, and in conjunction with mild, non-fragranced soaps or cleansing lotions, the condition can be made more comfortable for the child.
Topically applied soothing lotions or creams are often best chosen from the many homoeopathic lines now available in pharmacy, in preference to the favoured corticosteroid based creams.

The long term usage of these prescription products have their own inherent problems, and have proven detrimental affects on the skin of children.
In addition to rendering the skin light sensitive, with extended use they have been shown to impart thinning effects on the stratum corneum. In worst-case scenarios, the original condition can often return worse than before.
Baby Skin Care Products:
Infant skin, with the characteristics mentioned earlier, requires skin care different to that for adults.
Adult skin is divided into various skin types and conditions according to the lifelong effects of factors such as environment, work / play lifestyle, diseases and constitution.
Infant skin shows less differentiation than adult skin: the properties of infant skin vary little from one individual to the next.
All babies experience a big change in their skin characteristics a short time after birth, and with this in mind, the most appropriate skin care for babies would be one that takes greater account of the number of months since birth, rather than any individual skin differences.
Stay Notified
Sign up for news on topics of interest that will help you grow your career and our new releases.